Patent application title: METHODS AND APPARATUS FOR TREATING PULMONARY EMBOLISM
Inventors:
Robert Rosenbluth (Laguna Niguel, CA, US)
Robert Rosenbluth (Laguna Niguel, CA, US)
Paul Lubock (Monarch Beach, CA, US)
Brian J. Cox (Laguna Niguel, CA, US)
Richard Quick (Mission Viejo, CA, US)
Richard Quick (Mission Viejo, CA, US)
IPC8 Class: AA61F201FI
USPC Class:
600200
Class name: Laryngoscope illuminating otoscope (e.g., funnel shaped specula)
Publication date: 2016-05-26
Patent application number: 20160143721
Abstract:
A device and method for intravascular treatment of an embolism is
disclosed herein. One aspect of the present technology, for example, is
directed toward a clot treatment device that includes a support member
configured to extend through a delivery catheter and a plurality of clot
engagement members positioned about the circumference of a distal portion
of the support member. The clot engagement members can be configured to
penetrate clot material along an arcuate path and mechanically macerate
clot and release embolic particles when re-sheathed into the delivery
catheter.Claims:
1. A clot treatment device for treating a pulmonary embolism within a
blood vessel, the clot treatment device being moveable between a
low-profile undeployed state and a deployed state, the clot treatment
device comprising: a support member configured to extend through a
delivery catheter, wherein the support member has a proximal portion and
a distal portion; a plurality of clot engagement members positioned
circumferentially about at least an area of the distal portion of the
support member, wherein individual clot engagement members have a curved
portion; wherein the clot engagement members are configured to penetrate
clot material along an arcuate path and mechanically macerate clot
material and release embolic particles when re-sheathed into the delivery
catheter.
2. The clot treatment device of claim 1 wherein, in the deployed state, individual curved portions of the clot engagement members project radially outwardly relative to the support member in a curve that has a proximally extending section which defines a proximally facing concave portion, and wherein the individual curved portions further include an end section that curves radially inwardly from the proximally extending section.
3. A method of treating a pulmonary embolism, comprising: accessing a venous vessel of a patient; inserting a catheter in the vessel and urging the catheter through the vessel, through chambers of the patient's heart and into a pulmonary artery until a distal end of the catheter is located at a region distal of a pulmonary embolism; delivering a treatment device having a plurality of radially extending members through the catheter; disturbing the embolus by mechanical maceration of the embolus to release embolic particles without capturing the embolic particles in an embolic protection device; and establishing one or more blood flow channels through the embolus wherein the one or more blood flow channels facilitate natural lysis of the embolus.
4. A method of treating a pulmonary embolism comprising: delivering an embolectomy device through the heart to a pulmonary embolism that at least partially restricts blood flow through a pulmonary vessel, wherein the embolectomy device comprises an expandable cylindrical section and a radial expansion member configured to expand outwardly from the cylindrical section; deploying the embolectomy device within the pulmonary embolism so as to restore blood flow through said pulmonary embolism, wherein deploying the embolectomy device comprises expanding the cylindrical section within the pulmonary embolism such that the cylindrical section forms an expanded flow channel through the pulmonary embolism and expanding the radial expansion member to a greater extent than the cylindrical section, and wherein at full expansion of the cylindrical member the radial expansion member projects outward from the cylindrical member; fragmenting the pulmonary embolism while moving the embolectomy device and at least a portion of the pulmonary embolism along the pulmonary vessel; and withdrawing the embolectomy device and at least a portion of the pulmonary embolism from the pulmonary vessel.
5. A device for treating a pulmonary embolism that at least partially restricts blood flow through a pulmonary vessel, the device comprising: an elongated shaft having a proximal region and a distal region; an expandable braid attached to the distal region of the elongated shaft, the braid having a plurality of radially extending portions and at least one cylindrical portion, and the radially extending portions and the cylindrical portion being configured to move from a compressed state sized to fit in a delivery catheter to an expanded state; wherein the cylindrical portion is between a pair of the radially extending portions, and in the expanded state the cylindrical portion is configured to press radially outward against the pulmonary embolism; wherein the radially extending portions extend radially outward from the cylindrical portion in the expanded state such that portions of the pulmonary embolism are retained between the radially extending portions; and wherein the cylindrical portion has a first length along a longitudinal direction of the braid in the expanded state and the radially extending portions have a second length along the longitudinal direction of the braid in the expanded state that is less that the first length; and wherein the radially extending portions and/or the cylindrical portions are configured to elongate and/or contract when re-sheathed into the delivery catheter to mechanically macerate clot and release embolic particles.
6. The device of claim 1 wherein at least a portion of the individual radially extending portions is disk-shaped.
7. The device of claim 1 wherein the individual radially extending portions include a curved portion and a linear portion.
Description:
CROSS-REFERENCE TO RELATED APPLICATIONS
[0001] The present application claims the benefit of U.S. Provisional Patent Application No. 61/845,796, filed Jul. 12, 2013, entitled "DEVICES AND METHODS FOR TREATING OF VASCULAR OCCLUSION", U.S. Provisional Patent Application No. 61/864,356, filed Aug. 9, 2013, entitled "DEVICES AND METHODS FOR TREATING OF VASCULAR OCCLUSION", U.S. Provisional Patent Application No. 61/949,953 filed Mar. 7, 2014, entitled "METHODS AND APPARATUS FOR TREATING EMBOLISM," and U.S. patent application Ser. No. 14/299,933, filed Jun. 9, 2014, entitled "METHODS AND APPARATUS FOR TREATING PULMONARY EMBOLISM", all of which are incorporated herein by reference in their entireties.
TECHNICAL FIELD
[0002] The present technology relates generally to devices and methods for intravascular treatment of emboli within a blood vessel of a human patient. Many embodiments of the technology relate to the intravascular treatment of a pulmonary embolism.
BACKGROUND
[0003] Thromboembolism occurs when a thrombus or blood clot trapped within a blood vessel breaks loose and travels through the blood stream to another location in the circulatory system, resulting in a clot or obstruction at the new location. As shown schematically in FIG. 1, when a clot C forms in the venous circulation V, it often travels to the lungs L via the heart H and lodges within a pulmonary blood vessel PV causing a pulmonary embolism PE. A pulmonary embolism PE can decrease blood flow through the lungs L, which in turn causes decreased oxygenation of the lungs L, heart H and rest of the body. Moreover, pulmonary embolisms can cause the right ventricle RV of the heart H to pump harder to provide sufficient blood to the pulmonary blood vessels PV, which can cause right ventricle RV dysfunction (dilation), and heart failure in more extreme cases.
[0004] Conventional approaches to treating thromboembolism and/or pulmonary embolism include clot reduction and/or removal. For example, anticoagulants can be introduced to the affected vessel to prevent additional clots from forming, and thrombolytics can be introduced to the vessel to at least partially disintegrate the clot. However, such agents typically take a prolonged period of time (e.g., hours, days, etc.) before the treatment is effective and in some instances can cause hemorrhaging. Transcatheter clot removal devices also exist, however, such devices are typically highly complex, prone to cause trauma to the vessel, hard to navigate to the pulmonary embolism site, and/or expensive to manufacture. Conventional approaches also include surgical techniques that involve opening the chest cavity and dissecting the pulmonary vessel. Such surgical procedures, however, come with increased cost, procedure time, risk of infection, higher morbidity, higher mortality, and recovery time. Accordingly, there is a need for devices and methods that address one or more of these deficiencies.
BRIEF DESCRIPTION OF THE DRAWINGS
[0005] Many aspects of the present technology can be better understood with reference to the following drawings. The components in the drawings are not necessarily to scale. Instead, emphasis is placed on illustrating clearly the principles of the present disclosure.
[0006] FIG. 1 is a schematic illustration of an embolism traveling through the heart and forming an embolism in a pulmonary vessel.
[0007] FIG. 2A is a perspective view of one embodiment of a clot treatment device in a collapsed or delivery state configured in accordance with an embodiment of the present technology.
[0008] FIG. 2B is a perspective view of the clot treatment device of FIG. 2A in a deployed state configured in accordance with an embodiment of the present technology.
[0009] FIG. 2C is an enlarged view of a portion the clot treatment device shown in FIG. 2A.
[0010] FIG. 2D is an axial-perspective view of a portion of the clot treatment device shown in FIG. 2A.
[0011] FIGS. 3A-3C are isolated, enlarged side views of clot engagement members in a deployed state configured in accordance with embodiments of the present technology.
[0012] FIG. 4A is a perspective view of another embodiment of a clot treatment device in a collapsed or delivery state configured in accordance with an embodiment of the present technology.
[0013] FIG. 4B is a perspective view of the clot treatment device of FIG. 4A in a deployed state configured in accordance with an embodiment of the present technology.
[0014] FIG. 5 is a perspective view of a clot treatment device configured in accordance with another embodiment of the present technology.
[0015] FIG. 6 is a perspective view of a clot treatment device configured in accordance with another embodiment of the present technology.
[0016] FIG. 7A is a perspective view of a clot treatment device configured in accordance with another embodiment of the present technology.
[0017] FIG. 7B is a cross-sectional end view taken along line 7B-7B in FIG. 7A.
[0018] FIG. 8 is a perspective view of a clot treatment device configured in accordance with another embodiment of the present technology.
[0019] FIG. 9A is a perspective view of a clot treatment device configured in accordance with another embodiment of the present technology.
[0020] FIG. 9B is a cross-sectional end view of a portion of the clot treatment device shown in FIG. 9A.
[0021] FIG. 9C is a side view of a binding member configured in accordance with the present technology.
[0022] FIG. 10 is a side partial cross-sectional view of a delivery system configured in accordance an embodiment of the present technology.
[0023] FIGS. 11A-11K illustrate a method for using a clot treatment device configured in accordance with the present technology to remove clot material from a vessel.
[0024] FIG. 12 is a cross-sectional view of a preferred embodiment of a clot treatment device in accordance with the present invention in a compressed, undeployed state;
[0025] FIG. 13 is a top view of a preferred embodiment of a clot treatment device in accordance with the present invention;
[0026] FIGS. 14A-14F are a series of cross-sectional views of a preferred embodiment of the method and device of the present invention;
[0027] FIGS. 15A-15B are a series of cross-sectional views of a preferred embodiment of the method and device of the present invention;
[0028] FIG. 16 is a cross-sectional view of another preferred embodiment of the method and device of the present invention; and,
[0029] FIGS. 17A-17H show cross-sectional views of preferred embodiments of a clot treatment device in accordance with the present invention.
[0030] FIG. 18 is a cross-sectional view of a clot treatment device in accordance with another embodiment of the present technology.
[0031] FIGS. 19 and 20 are detailed cross-sectional views of a distal portion and a proximal portion, respectively, of an expandable member of a clot treatment device in accordance with an embodiment of the present technology.
[0032] FIGS. 21 and 22 are detailed cross-sectional views of a proximal portion and a distal portion, respectively, of an expandable member of a clot treatment device in accordance with another embodiment of the technology.
[0033] FIGS. 23-26 are side views of guide members for use with clot treatment devices and methods in accordance with embodiments of the present technology.
DETAILED DESCRIPTION
[0034] Specific details of several embodiments of clot treatment devices, systems and associated methods in accordance with the present technology are described below with reference to FIGS. 2A-26. Although many of the embodiments are described below with respect to devices, systems, and methods for treating a pulmonary embolism, other applications and other embodiments in addition to those described herein are within the scope of the technology. Additionally, several other embodiments of the technology can have different states, components, or procedures than those described herein. Moreover, it will be appreciated that specific elements, substructures, advantages, uses, and/or other features of the embodiments described with reference to FIGS. 2A-26 can be suitably interchanged, substituted or otherwise configured with one another in accordance with additional embodiments of the present technology. Furthermore, suitable elements of the embodiments described with reference to FIGS. 2A-26 can be used as standalone and/or self-contained devices. A person of ordinary skill in the art, therefore, will accordingly understand that the technology can have other embodiments with additional elements, or the technology can have other embodiments without several of the features shown and described below with reference to FIGS. 2A-26.
[0035] With regard to the terms "distal" and "proximal" within this description, unless otherwise specified, the terms can reference a relative position of the portions of a clot treatment device and/or an associated delivery device with reference to an operator and/or a location in the vasculature.
I. Selected Embodiments of Clot Treatment Devices
[0036] FIG. 2A is a perspective view of one embodiment of a clot treatment device 200 ("the device 200") in a low-profile or delivery state, and FIG. 2B is a perspective view of the device 200 in an unrestricted expanded or deployed state that is well suited for removing clot material from a blood vessel (e.g., a pulmonary blood vessel). Referring to FIGS. 2A and 2B together, the device 200 can include a support member 204 and a plurality of clot engagement members 202 positioned about the circumference of the support member 204. As best shown in FIG. 2B, the individual clot engagement members 202 can include a first portion 206 having a proximal region 205 and a distal region 207, and a second portion 208 extending from the distal region 207 of the first portion 206. In the delivery state, as shown in FIG. 2A, the clot engagement members 202 can be generally linear and extend generally parallel to the support member 204. In the expanded state, as shown in FIG. 2B, the second portions 208 can project radially outwardly relative to the support member 204 in a curved shape. The second portions 208 can have a proximally facing section 212 which defines a proximally facing concave portion, and, in some embodiments, the second portions 208 can further include an end section 214 that curves radially inwardly from the proximally facing section 212. When deployed within a blood vessel adjacent to clot material, the clot engagement members 202 are configured to penetrate the clot material along an arcuate path and hold clot material to the device 200, as discussed in greater detail below with reference to FIGS. 10-11K.
[0037] FIG. 2C is an enlarged view of a portion of the device 200 of FIG. 2A showing that the device 200 can include a hub 210 that couples the proximal regions 205 of the first portions 206 to the support member 204. The first portions 206 can extend distally from their proximal regions 205 in a longitudinal direction along the length of the support member 204 to their distal regions 207, and the distal regions 207 can be free to move relative to the support member 204. As such, the first portions 206 can be cantilevered portions of the clot engagement members 202 that enable the clot engagement members 202 to flex and move independently of the support member 204 in response to forces present within the blood vessel, such as blood flow, gravity, and/or the local anatomy. The first portions 206 can be sufficiently rigid to maintain a generally linear shape along their respective lengths, yet flexible enough to bend and/or flex about the hub 210. For example, in some instances, in response to local forces, one or more of the distal regions 207 of the first portions 206 can be spaced radially apart from the support member 204 such that one or more first portions 206 forms an angle with the support member 204.
[0038] Referring back to FIGS. 2A and 2B, the first portions 206 of different clot engagement members 202 can have different lengths such that the second portions 208 of at least two clot engagement members extend radially outwardly at different locations along the length of the support member 204. For example, as best shown in FIG. 2B, the clot treatment device 200 can include a first group 202a of clot engagement members 202 having first portions 206 with a first length L1, a second group 202b of clot engagement members 202 having first portions 206 with a second length L2 greater than the first length L1, a third group of clot engagement members 202c having first portions 206 with a third length L3 greater than the second length L2, a fourth group of clot engagement members 202d having first portions 206 with a fourth length L4 greater than the third length L3, a fifth group of clot engagement members 202e having first portions 206 with a fifth length L5 greater than the fourth length L4, and a sixth group of clot engagement members 202f having first portions 206 with a sixth length L6 greater than the fifth length L5. It will be appreciated that although six groups of clot engagement members are shown in FIGS. 2A and 2B, in other embodiments the clot treatment device can have more or fewer than six groups (e.g., one group, two groups, three groups, seven groups, ten groups, etc.) and/or the lengths of all or some of the first portions 206 can be the same or different.
[0039] Moreover, the second portions 208 of the first group 202a of clot engagement members 202 extend radially outward at a first area of the support member 204, the second portions 208 of the second group 202b of the clot engagement members 202 extend radially outward from a second area of the support member 204, the second portions 208 of the third group 202c of clot engagement members 202 extend radially outward from a third area of the support member 204, the second portions 208 of the fourth group 202d of clot engagement members 202 extend radially outward from a fourth area of the support member 204, the second portions 208 of the fifth group 202e of clot engagement members 202 extend radially outward from a fifth area of the support member 204, and the second portions 208 of the sixth group 202f of clot engagement members 202 extend radially outward from a sixth area of the support member 204. It will be appreciated that although six areas of clot engagement members are shown in FIGS. 2A and 2B, in other embodiments the clot treatment device can have more or fewer than six areas (e.g., one area, two areas, three areas, five areas, nine areas, etc.).
[0040] FIG. 2D is an enlarged, axial-perspective view of a portion of the device 200 in which the groups of clot engagement members 202a-f (only the first, second and third groups 202a-c shown) are arranged about the circumference of the support member 204 such that the second portions (labeled 208a-c) of adjacent groups 202a-c are circumferentially offset from one another. As such, in the embodiment shown in FIG. 2D, the second portions 208 of adjacent groups of clot engagement members 202a-f are not circumferentially aligned, and thus can engage the clot material at different circumferential positions along the length of the clot material.
[0041] FIG. 3A is a side view of a clot engagement member 202 in the expanded state. Individual clot engagement members can be made from a shape memory material such that, when unconstrained, assume a preformed curved shape. As shown in FIG. 3A, the second portion 208 can have an arcuate shape that includes an outwardly extending section 216, the proximally facing section 212 extending from the outwardly extending section 216, and the end section 214 extending from the proximally facing section 212. In one embodiment, the demarcation between the proximally facing section 212 and the end section 214 occurs at an apex 218 of the second portion 208. The proximally facing section 212 is configured to retain clot material with the clot engagement member 202 as the device 200 is pulled proximally through the vessel (arrow P), and the apex 218 provides a smooth curve that can atraumatically slide along the vessel wall as the device 200 is pulled proximally through the vessel. In the embodiment shown in FIG. 3A, the second portion 208 of the clot treatment device 200 can have a single or constant radius of curvature R1. In other embodiments, such as the clot engagement member 402 shown in FIG. 3B, the second portions 208 can have a plurality of radii of curvature, such as a first region with a first radius of curvature R1 and a second region with a second radius of curvature R2. In the embodiment shown in FIGS. 2A-2D, the second portions 208 of the clot engagement members 202 have a single radius of curvature that is the same for all of the clot engagement members 202. In other embodiments, the device 200 can have a first group of second portions with a constant radius of curvature and a second group of second portions with a plurality of radii of curvature. Moreover, in additional embodiments the device 200 can include a first group of second portions having a first radius of curvature and a second group of second portions having a second radius of curvature different than the first radius of curvature. In some embodiments, the radius R1 of the clot engagement members 202 can be between about 1.5 mm and about 12 mm, and in some embodiments, between about 2 mm and about 12 mm.
[0042] As shown in FIG. 3C, the arc length a of the clot engagement members 202 may be substantially greater than 180 degrees to provide several benefits in performance of clot engagement and retrieval. In particular, a greater arc length a can provide improved clot engagement during retraction when resistance due to clot friction and interference with the vessel wall deflects the clot engagement member 202 distally (arrow D). A greater arc length a may provide more deflection and/or unravelling or straightening of the arcuate shape without loss of engagement with the clot. In some embodiments, the arc length a of the clot engagement members 202 can be greater than about 200 degrees. In some embodiments the arc length a of the clot engagement members 202 may be between about 200 degrees and 340 degrees and between about 240 degrees and 300 degrees in other embodiments. It can be advantageous to keep the arc length a under about 360 degrees so as to avoid overlap of the clot engagement member 202. Greater arc length a can allow for the use of smaller clot engagement member filaments or wires that may be particularly beneficial for minimization of the collapsed profile of the device. Greater arc length a can also allow for a larger total number of clot engagement members 202 that also enhance the ability of the device to remove embolic material from a vessel. Moreover, in some embodiments, the distal end of the clot engagement members 202 may define an angle with respect to the axis of the support member and/or the straight portion of the engagement members (as shown in FIG. 3C). This angle may be between about 30 degrees and about 90 degrees, and in some embodiments between about 40 degrees and about 80 degrees.
[0043] The clot engagement members 202 can be made from a variety of materials. In a particular embodiment, the clot engagement members 202 comprise a material with sufficient elasticity to allow for repeated collapse into an appropriately sized catheter and full deployment in a blood vessel. Such suitable metals can include nickel-titanium alloys (e.g., Nitinol), platinum, cobalt-chrome alloys, Elgiloy, stainless steel, tungsten, titanium and/or others. Polymers and metal/polymer composites can also be utilized in the construction of the clot engagement members. Polymer materials can include Dacron, polyester, polyethylene, polypropylene, nylon, Teflon, PTFE, ePTFE, TFE, PET, TPE, PLA silicone, polyurethane, polyethylene, ABS, polycarbonate, styrene, polyimide, PEBAX, Hytrel, polyvinyl chloride, HDPE, LDPE, PEEK, rubber, latex and the like. In some embodiments, the clot engagement members 202 may comprise an environmentally responsive material, also known as a smart material. Smart materials are designed materials that have one or more properties that can be significantly changed in a controlled fashion by external stimuli, such as stress, temperature, moisture, pH, electric or magnetic fields.
[0044] In some embodiments, portions of the exterior surfaces of the support member 204 and/or clot engagement members 202 may be textured, or the exterior surfaces can include microfeatures configured to facilitate engagement or adhesion of thrombus material (e.g., ridges, bumps, protrusions, grooves, cut-outs, recesses, serrations, etc.). In some embodiments, the clot engagement members 202 may be coated with one or more materials to promote platelet activation or adhesion of thrombus material. Adhesion of thrombi to clot engagement members 202 may facilitate capture and/or removal.
[0045] In some embodiments, the clot treatment device 200 can include between about 8 and about 80 clot engagement members 202, and in some embodiments, between about 12 and about 60 clot engagement members 202. In a particular embodiment, the clot treatment device 200 can include between about 16 and about 40 clot engagement members 202. The clot engagement members 202 can individually have one consistent diameter or have a variety of diameters (among the members 202) along their lengths. In addition, an individual clot engagement member 202 may have a tapered or varying diameter along its length to provide desired mechanical characteristics. The average diameter of the clot engagement members 202 can be between about 0.1 mm to about 0.2 mm in some embodiments and in a particular embodiment, between about 0.12 mm and 0.16 mm.
[0046] In any of the embodiments described herein, the clot engagement members 202 can be formed from a filament or wire having a circular cross-section. Additionally, the clot engagement members 202 can be formed from a filament or wire having a non-circular cross-section. For example, filaments or wires having square, rectangular and oval cross-sections may be used. In some embodiments, a rectangular wire (also known as a "flat wire") may have a height or radial dimension of between about 0.05 mm to about 0.2 mm. In some embodiments, a rectangular wire may have a width or transverse dimension of between about 0.08 mm to about 0.3 mm. In some embodiments, a rectangular wire may have a height to width ratio of between about 0.3 to about 0.9 and between about 1 and about 1.8.
[0047] FIGS. 4A and 4B illustrate an embodiment in which clot engagement members having non-circular cross-sections are fabricated from a tube (e.g., a hypotube). The tube may be cut or machined by various means known in the art including conventional machining, laser cutting, electrical discharge machining (EDM) or photochemical machining (PCM). Referring to FIG. 4A, a tube may be cut to form a plurality of clot engagement members 454 that are integral with a hub member 456. The cut tube may then be formed by heat treatment to move from a delivery state shown in FIG. 4A to a deployed state shown in FIG. 4B in which an array of arcuate clot engagement members 454 project radially outward. As is known in the art of heat setting, a fixture or mold may be used to hold the structure in its desired final configuration and subjected to an appropriate heat treatment such that the clot engagement members assume or are otherwise shape-set to the desire arcuate shape. In some embodiments, the device or component may be held by a fixture and heated to about 475-525° C. for about 5-15 minutes to shape-set the structure. In some embodiments, the tubular clot engagement structure may be formed from various metals or alloys such as Nitinol, platinum, cobalt-chrome alloys, 35N LT, Elgiloy, stainless steel, tungsten or titanium.
[0048] FIG. 5 is a perspective view of another embodiment of a clot treatment device 500 in a deployed state in accordance with the present technology. As shown in FIG. 5, the clot treatment device 500 can include a plurality of clot engagement members 502 generally similar to the clot engagement members 202 and 402 described with reference to FIGS. 2A-4B, except the clot engagement members 502 of FIG. 5 are arranged about the support member 204 such that the length of the first portions 506 increase in a clockwise or counterclockwise direction about 360 degrees of the support member 204. As such, the second portions 508 spiral around the length of the support member 204 and each successive second portion 508 extends from a location along the shaft that is circumferentially offset and distal to the location of the immediately adjacent second portion 508.
[0049] FIG. 6 is a perspective view of another embodiment of a clot treatment device 600 in a deployed state in accordance with the present technology. The clot treatment device 600 can include a plurality of clot engagement members 602 generally similar to the clot engagement members 202 and 402 described with reference to FIGS. 2A-4B, except the second portions 608 of the clot engagement members 602 of FIG. 6 are not arranged in groups, but instead extend at irregular intervals from support member 204.
[0050] FIG. 7A is a perspective view of another embodiment of a clot treatment device 700 in a deployed state in accordance with the present technology, and FIG. 7B is a cross-sectional end view taken along line 7B-7B in FIG. 7A. Referring to FIGS. 7A and 7B together, the clot treatment device 700 can have groups of clot engagement members 702a-f spaced along the support member 204. The groups 702a-f can include a plurality of arcuate clot engagement members 702 generally similar to the clot engagement members 202 and 402 described with reference to FIGS. 2A-4B, except the second portions 708 of the clot engagement members 702 of FIG. 7A extend at an angle from the support member 204 such that the distal ends 713 of the second portions 708 are not circumferentially aligned with the corresponding proximal ends 711 of the second portions 708. For example, as shown in FIG. 7B, the second portions 708 can extend at an angle θ from the first portions 706. In some embodiments, the angle θ can be between about 10 and about 80 degrees. In a particular embodiment, the angle θ can be between about 40 and about 60 degrees. Additionally, as shown in FIGS. 4B and 7B, the clot engagement members may form a substantially circular axial array about the axis of the support member. A circular array may engage clot more uniformly and securely than a non-circular array and thus may facilitate retrieval and removal of clot from the vessel.
[0051] FIG. 8 is a perspective view of another embodiment of a clot treatment device 800 in a deployed state in accordance with the present technology. As shown in FIG. 8, the clot treatment device 800 can have groups of clot engagement members 802a-f spaced along the support member 204. The groups 802a-f can include a plurality of arcuate clot engagement members 802 generally similar to the clot engagement members 202 and 402 described with reference to FIGS. 2A-4B, except the clot engagement members 802 of FIG. 8 do not include a first or cantilevered portion. As such, the clot engagement members 802 include only a curved second portion 808 which is coupled to the support member 204 at one end (e.g., via hubs 810a-f). In a particular embodiment, the clot engagement members 802 can have a first portion; however, in such embodiments, the first portions of the clot engagement members 802 are relatively short (e.g., less than about 10 mm) In some embodiments, the groups 802a-f can be evenly spaced along the support member 204, and in other embodiments the groups 802a-f can have any spacing or state along the support member 204. Additionally, the arcuate clot engagement members 802 at one group 802 can have a different size than the arcuate clot engagement members 802 at a different group 802. The groups 802a-f can be deployed or expanded simultaneously (e.g., via a push-wire or other deployment methods) or consecutively (e.g., by retracting a sheath).
[0052] FIG. 9A is a perspective view of another embodiment of a clot treatment device 950 in a deployed state configured in accordance with the present technology. In some embodiments, the device 950 can include a plurality of clot engagement members 952 arranged in closely-packed circular array. The clot engagement members 952 can be generally similar to the clot engagement members 202 and 402 described with reference to FIGS. 2A-4B. A proximal portion of the clot engagement members 952 can be bound together and surrounded by a tubular binding member 960. The clot engagement members 952 can fill substantially all of a lumen of the binding member 960, as shown in the cross-sectional view of FIG. 9B (other than the small gaps between the clot engagement members (that are too small for another clot engagement member)). In another embodiment (not shown), a lumen or tube may provide for passage of a guidewire or catheter through the bundle of clot engagement members. Referring to FIG. 9A, the clot engagement members 952 can have first portions 956 with differing lengths so that the second portions 956 are spread out over a deployed engagement member length L. In some embodiments, the deployed engagement member length L may be between about 0.5 cm and about 8 cm, and in some embodiments, between about 1 cm and about 5 cm. As shown in FIG. 9C, the binding member 960 can be a coil, spiral, tube, sleeve, braid and/or other generally suitable tubular configurations. The binding member 960 may be slotted, cut or otherwise fenestrated to enhance flexibility. The binding member 960 may be made of various metals, polymers and combinations thereof and may comprise materials visible under x-ray or fluoroscopy so as to function as a radiopaque marker to facilitate deployment, placement and retraction by the user.
[0053] FIG. 10 is a side partial cross-sectional view of one embodiment of a delivery system 910 for delivering the clot treatment device 200 to a treatment site, such as a pulmonary embolism. The delivery system 910 can include a proximal portion 911, an elongated delivery catheter 920 extending from a distal region of the proximal portion 911, a delivery sheath 930 slidably received within a lumen of the delivery catheter 920, a tubular push member 940 slidably received within a lumen of the delivery sheath 930, and a guidewire 912 slidably received within a lumen of the push member 940. As shown in FIG. 10, the clot treatment device 200 can be positioned within the delivery sheath 930 such that the delivery sheath 930 constrains the clot engagement members 202 in a low-profile delivery state that is generally parallel with the support member 204. In some embodiments, the delivery catheter 920 can have an outside diameter between about 0.8 mm and about 1.8 mm, and in some embodiments, between about 0.1 mm and about 0.16 mm. A proximal portion of the support member 204 can be coupled to a distal region of the push member 204 such that axial movement of the push member 204 causes axial movement of the support member 204 (and thus the clot treatment device 200).
[0054] The proximal portion 911 of the device can include a first hub 922 and a second hub 932 configured to be positioned external to the patient. The first and/or second hubs 922, 932 can include a hemostatic adaptor, a Tuohy Borst adaptor, and/or other suitable valves and/or sealing devices. A distal region 920a of the first hub 922 can be coupled to the delivery catheter 920, and a proximal region of the first hub 922 can include an opening 924 configured to slidably receive the delivery sheath 930 therethrough. In some embodiments, the first hub 922 can further include an aspiration line 926 coupled to a negative pressure-generating device 928 (shown schematically), such as a syringe or a vacuum pump. A distal region 932a of the second hub 932 can be fixed to a proximal region of the delivery sheath 930, and a proximal region of the second hub 932 can include an opening 934 configured to receive the push member 940 therethrough. Additionally, in some embodiments, the second hub 932 can include a port 936 configured to receive one or more fluids before, during and/or after the procedure (e.g., contrast, saline, etc.).
[0055] FIGS. 11A-11K illustrate one example for treating an embolism (e.g., a pulmonary embolism) with the clot treatment device 200 (and delivery system 910). FIG. 11A is a side view of a delivery system 910 positioned adjacent to an embolism or clot material PE within a pulmonary blood vessel V. Access to the pulmonary vessels can be achieved through the patient's vasculature, for example, via the femoral vein. The delivery system 910 can be guided through the right atrium, through the tricuspid valve, into the right ventricle, through the pulmonary valve and into the main pulmonary artery. Depending on the location of the embolism, the delivery system 910 can be guided to one or more of the branches of the right pulmonary artery and/or the left pulmonary artery. It will be understood, however, that other access locations into the venous circulatory system of a patient are possible and consistent with the present technology. For example, the user can gain access through the jugular vein, the subclavian vein, the brachial vein or any other vein that connects or eventually leads to the superior vena cava. Use of other vessels that are closer to the right atrium of the patient's heart can also be advantageous as it reduces the length of the instruments needed to reach the pulmonary embolism.
[0056] As shown in FIG. 11A, the delivery sheath 930 containing the collapsed clot treatment device 200 (not shown) can be advanced together with the delivery catheter 920 over the guidewire 912 to the treatment site. For example, the guidewire 912 can be inserted through the target pulmonary embolism PE. Referring to FIG. 11B, a distal portion of the delivery catheter 920 and/or delivery sheath 930 can then be advanced through the pulmonary embolism PE such that the distal ends 201 of at least one group of the clot engagement members 202 are aligned with or positioned distal to a distal edge of the pulmonary embolism PE. In other embodiments (not shown), a distal portion of the delivery catheter 920 and/or delivery sheath 930 can be positioned such that the distal ends 201 of at least one group of the clot engagement members 202 are positioned proximal to a distal edge of the pulmonary embolism PE.
[0057] Once the device is positioned, the guidewire 912 can then be removed proximally through a lumen of the delivery sheath 930 and/or delivery catheter 920, and the delivery sheath 930 can be pulled proximally to a position proximal of the pulmonary embolism PE (as shown in FIG. 11B). As shown in FIGS. 11C-11G, the delivery sheath 930 can be retracted proximally to expose the distal portions of the second portions 208 of the clot engagement members such that the exposed portions radially expand and bend backwards in a proximal direction. As the second portions 208 expand, they extend into the pulmonary embolism PE around the device along an arcuate path P. The arcuate path P can extend radially outward and proximally with respect to the support member (not shown) and, as shown in FIG. 11F, can eventually curve radially inwardly. The second portions 208 can thus form hook-like capture elements that penetrate into and hold clot material to the device 200 for subsequent removal. Moreover, should the second portions 208 extend radially outwardly enough to touch the vessel wall, the end sections 214 of the second portions 208 form an atraumatic surface that can abut or apply pressure to the vessel wall without damaging the vessel wall. In some embodiments, the device presents a plurality of arcuate members that may be substantially parallel with the axis of the device at the point of contact with the vessel wall when in the deployed state.
[0058] Still referring to FIG. 11F, when the delivery sheath 930 is withdrawn proximally beyond the second portions 208 of the most distal group of clot engagement members 202f, the first portions 206 of the clot engagement members 202f are exposed. In some embodiments, the delivery sheath 930 can be withdrawn so as to expose only a portion of the clot engagement members. Additionally, in those embodiments having two or more groups of clot engagement members, the delivery sheath 930 can be withdrawn to expose all or some of the groups of clot engagement members. As shown in FIG. 11G, the delivery sheath 930 can continue to be withdrawn proximally to expose additional second portions 208 and/or groups of clot engagement members 202a-f. Clot engagement members 202a-f may just contact or be slightly deflected by the vessel wall. If the device is sized such that the diameter of the clot engagement members are larger than the vessel diameter (e.g., "over-sized"), the clot engagement members may be compressed by the vessel wall. Thus, while fully deployed, the device may be in state of a small amount of radial compression. In some embodiments, the device may be diametrically over-sized by between about 5% and 50% and in other embodiments between about 10% and 25%.
[0059] As shown in FIGS. 11H-11K, once at least a portion of the clot engagement members and/or second portions 208 have penetrated and engaged the targeted clot material PE, the clot treatment device 200 can be withdrawn proximally, thereby pulling at least a portion of the clot material PE in a proximal direction with the device 200. For example, the push member 940, second hub 932, and delivery sheath 930 (FIG. 10) can be retracted proximally at the same time and rate. As such, the delivery catheter 920 can be held in place while the delivery sheath 930, clot material PE, and clot treatment device 200 are pulled proximally into the delivery catheter 920. The curved shape of the second portions 208 increases the surface area of the clot engagement members 202 in contact with the clot material PE, thus increasing the proximal forces exerted on the clot material. Withdrawal of the device 200 not only removes the clot but also can increase blood flow through the vessel.
[0060] As shown in FIG. 11K, in some embodiments the delivery catheter 920 can include an aspiration lumen (not shown) configured to apply a negative pressure (indicated by arrows A) to facilitate removal of the clot material PE. For example, the delivery catheter 920, delivery sheath 930 and/or clot treatment device 200 of the present technology can be configured to be operably coupled to the retraction and aspiration apparatus disclosed in Attorney Docket No. 111552.8004.US00, titled "Retraction and Aspiration Apparatus and Associated Systems and Methods," filed concurrently herewith, which is incorporated herein by reference in its entirety. When coupled to the retraction and aspiration apparatus, a negative pressure is applied at or near the distal portion of the delivery catheter 920 (via the aspiration lumen) only while the clot treatment device 200 and/or delivery sheath 930 is being retracted. Therefore, when retraction pauses or stops altogether, aspiration also pauses or stops altogether. Accordingly, aspiration is non-continuous and dependent upon retraction of the delivery sheath 930 and/or clot treatment device 200. Such non-continuous, synchronized aspiration and retraction can be advantageous because it reduces the amount of fluid withdrawn from the patient's body during treatment (and thus less fluid need be replaced, if necessary). In addition, it may be advantageous to consolidate the steps and motions required to both mechanically transport thrombus into the guide catheter (e.g. aspiration tube) and remove fluid from the tube into one motion, by one person.
II. Additional Selected Embodiments of Clot Treatment Devices
[0061] FIG. 12 shows an enlarged, side view of one embodiment of a clot treatment device 1202 (also referred to as "the device 1202") configured in accordance with the present technology, shown in a low-profile or delivery state and constrained within a delivery catheter 1406. FIG. 13 shows the device 1202 of FIG. 12 in an expanded or deployed state after removal of the delivery catheter 1406. As described in greater detail below, the clot treatment device 1202 can be delivered to a clot at a treatment site to restore blood flow through the clot and remove at least a portion of the clot. Referring to FIGS. 12 and 13 together, the device 1202 can be made of a self-expanding mesh or braided material such as a wire lattice, wire braid and/or stent. The material can be superelastic (e.g., Nitinol) or an alternative material such as a cobalt chrome alloy. It is believed that that porous structure of the clot treatment device 1202 allows for the flow of blood through the device 1202 during treatment, thus creating a lumen through the clot material that restores significant blood flow across the clot.
[0062] The clot treatment device 1202 can have distal ends coupled to an atraumatic distal hub 1205 and proximal ends coupled to proximal hub 1203. The proximal hub 1203 can be coupled to an elongated pusher member 1201 (shown in FIG. 13), such as an elongated rod, wire, or tubular coil. In some embodiments, the clot treatment device 1202 can be an "over the wire" device. In such embodiments, the pusher member 1201 can have a lumen, and the proximal hub 1203 and/or the distal hub 1205 can have a hollow, central lumen for receiving a guide wire. In these and other embodiments, the distal portion of the clot treatment device 1202 can have a flexible, atraumatic member (not shown) that extends distally from the device 1202. In yet further embodiments, the distal hub 1205 can be tapered to better penetrate the clot material in the vessel.
[0063] In some embodiments, the clot treatment device 1202 can have a generally cylindrical shape that, during use, provides a flow lumen for blood across a clot. The treatment device 1202 is not, however, limited to a generally cylindrical shape. For example, the shape can be generally conical, generally concave or generally convex along its axis, so long as such shapes provide the aforesaid lumen for blood flow.
[0064] Referring still to FIGS. 12 and 13, the clot treatment device 1202 is compressed to fit within the diameter DL of a lumen 1407 of the delivery catheter 1406 in the undeployed state. In the deployed state shown in FIG. 13, the clot treatment device 1202 has a plurality of capture elements, such as a series of radially extending capture portions 1206 which are separated from each other by flow restoration portions 1212. The flow restoration portions 1212 are configured to expand outwardly from the low-profile undeployed state within the delivery catheter lumen 1407 to a first cross-sectional dimension D1 (e.g., diameter) in the deployed state. For example, the flow restoration portions 1212 can be generally cylindrical braided sections that expand radially outward from the undeployed stated to the deployed state. In many applications, the first cross-sectional dimension D1 is greater than the diameter DL of the delivery catheter lumen 1407. The capture portions 1206 are configured to expand outwardly from the low-profile undeployed state to a second cross-sectional dimension D2 greater than the first cross-sectional dimension D1 in the deployed state. As explained in more detail below, the capture portions 1206 can project into the clot such that they extend transverse to a longitudinal axis L-L of the clot treatment device 1202, while the flow restoration portions 1212 expand radially outward into the clot to open a passage through which blood can quickly resume flow through the vessel. The clot treatment device 1202 can be porous so blood flows therethrough. In this regard, many embodiments of the clot treatment device 1202 are made from a mesh or braided material. The material can be a super-elastic material such as Nitinol or an alternative material such as cobalt chrome alloy. The device can be made from a wire lattice, wire braid or stent.
[0065] Referring again to FIG. 13, the clot treatment device 1202 can comprise a single mesh structure that is generally cylindrical in the low-profile undeployed state (shown in FIG. 12). The series of radially extending capture portions 1206 accordingly extend from the same mesh as the corresponding series of flow restoration portions 1212. The flow restoration portions 1212 can be generally cylindrical sections in the deployed state, or in other embodiments the flow restoration portions 1212 may taper in the distal direction individually and/or collectively to form a conical lumen (not shown). Each of the radially extending portions 1206 can be a radial or otherwise transversely projecting disk that projects outward relative to the flow restoration portions 1212.
[0066] FIGS. 14A-14F illustrate a method in accordance with the present technology for restoring flow and removing/retrieving clot material in a body lumen L using the clot treatment device 1202. Access to a treatment site, such as a clot E in a pulmonary vessel, can be achieved as described with reference to FIGS. 11A-11K. Upon delivery of the device 1202 to the treatment site, a guidewire 1402 can be extended through the clot E in the body lumen L as shown in FIG. 14A. As shown in FIG. 14B, a guide catheter 1404 can then be placed over the guidewire 1402 and moved to a location where a distal end of the guide catheter 1404 is positioned proximal to the clot E. At this point, the guidewire 1402 can optionally be withdrawn. However, in the embodiment shown in FIG. 14C, the guidewire 1402 can remain positioned through the clot and a delivery catheter 1406 can be moved through the guide catheter 1404 over the guidewire 1402 and pushed through the clot E. As shown in FIG. 14D, the guidewire 1402 can then be withdrawn, and the clot treatment device 1202 can be advanced distally through the delivery catheter 1406 until it is positioned at a distal portion of the delivery catheter 1406. Alternatively, if an over-the-wire device configuration is used, the guidewire 1402 can be left in place while the treatment device 1202 is deployed and retracted.
[0067] Referring to FIG. 14E, the delivery catheter 1406 can then be retracted in a proximal direction while maintaining forward pressure on the clot treatment device 1202 via the pusher member 1201 so that the clot treatment device 1202 becomes exposed and released from the delivery catheter 1406. The clot treatment device 1202 can radially expands into the clot E and, some embodiments, at least a portion of the clot treatment device 1202 expands distal of the clot E. For example, at least one of the radially extending capture portions 1206 of the clot treatment device 1202 is located distal to the clot E upon expansion of the device 1202. Additionally, the flow restoration portions 1212 between the capture portions 1206 also expand outwardly against a portion of the clot E to form a flow passage 1230 though the clot treatment device 1202.
[0068] The clot treatment device 1202 accordingly restores blood flow through the clot E immediately or at least quickly after expanding to the deployed state as shown by arrows 1207 in FIG. 14E. More specifically, the blood freely moves through the mesh of the clot treatment device 1202, travels through the device lumen and exits the clot treatment device 1202 distal to the clot E. As a result, the acute condition of blockage is mediated thus immediately improving the circulation of oxygenated blood in the patient.
[0069] The restoration of blood flow is anticipated to equate with restoration of a substantial portion of the normal blood flow rate for the patient. In less severe, e.g., "sub-massive" pulmonary embolism patients, the clot treatment device 1202 can increase blood flow rate by at least about 50 ml/min, at least about 150 ml/min or between about 100 to 250 ml/min. In severe, e.g., "massive" pulmonary embolism patients, a larger amount of the pulmonary artery flow is compromised. Hence, in some embodiments, at least about 500 ml/min of blood flow rate may be restored. Moreover, at least a portion of the flow restoration is expected to occur prior to the removal of the clot E, or any portion thereof.
[0070] The restoration of blood flow by the clot treatment device 1202 can be achieved in a low pressure environment. For example, the pressure in the target vessel can be less than 60 mmHg and the blood can be venous blood, substantially non-oxygenated blood or low oxygenated blood.
[0071] In addition to restoring blood flow, the expansion of the clot treatment device 1202 also impinges or cuts into the clot material. This enhances the subsequent removal of the clot E since portions of the clot E collect (1) between the capture portions 1206; (2) through the pores of the mesh forming the radially extending portions 1206; (3) along the longitudinal cylindrical sections 1212 between the capture portions 1206 of the treatment device 1202; and (4) within the clot treatment device 1202 itself.
[0072] As can be understood from the above description and the drawing figures, the deployment of the clot treatment device 1202 results in an outwardly expanding generally cylindrical force being urged against an inner surface of the clot E. This force pushes the clot material outwardly and creates a lumen through which blood flow is restored. As can also be appreciated, the presence of the radially extending portions 1206 on the clot treatment device 1202 causes the outwardly expanding generally cylindrical force to vary in magnitude along the axis of the clot treatment device 1202. The force on the clot material may be greater at the locations of the capture portions 1206.
[0073] In braided embodiments of the clot treatment device 1202, deployment of the device leads the filaments of the braid to change their angular orientation with respect to the axis of the device. This angular change may improve or enhance adherence of clot material to the clot treatment device 1202.
[0074] After the clot treatment device 1202 has been expanded and blood flow restored, the user then retracts the clot treatment device 1202 in a proximal direction as shown in FIG. 14F. Since the capture portions 1206 extend transverse to the longitudinal dimension of the vessel, the capture portions 1206 form transverse surfaces relative to the force exerted against the clot E as the clot treatment device 1202 is pulled in the proximal direction. The capture portions 406 accordingly enhance the ability of the clot treatment device 1202 to securely dislodge and retain the clot E as the clot treatment device 1202 and the delivery catheter 1406 are pulled back simultaneously into the guide catheter 1404. This is followed by the entire apparatus (e.g., clot treatment device 1202, delivery catheter 1406 and guide catheter 1404) being withdrawn through the heart and the venous circulation and out of the body.
[0075] As further shown in FIG. 14F, the clot treatment device 1202 may elongate as it is being withdrawn into the guide catheter 1404 due to the resistance it encounters from the presence of clot material of the clot E. The presence of the radially extending portions 1206 may allow elongation of the device 1202 that enhances the capability of the device 1202 to capture the maximum amount of clot material. This is further discussed below with respect to the surface area and expansion ratio of preferred embodiments of the clot treatment device 1202.
[0076] It will be appreciated that variations in the above-described method are contemplated. For example, in certain circumstances a guide catheter 1404 may not be necessary or desirable and the user may choose to use only the delivery catheter 1406 for placing and manipulation of the clot treatment device 1202. As a further example, the clot may be of such a nature that the user may desire repeat the above-described process, or at least portions of it, in order to more fully remove the clot E or clot material.
[0077] Referring next to FIGS. 15A-15B, it may be advantageous to include the use of a collection or funnel catheter 1412 to assist in the removal of the clot E. Such a funnel catheter 1412 has an expandable portion 1414 at its distal end and may be situated between the guide catheter 1404 and the delivery catheter 1406 or may be part of the guide catheter 1404. In the presence of the collection catheter 1412, the clot treatment device 1202 is pulled proximally into the collection catheter 1412 such that the clot or portions of it are captured within the collection catheter 1412. In an alternative embodiment, the collection catheter 1412 can be pushed distally over the clot treatment device 1202 and capture the clot, or portions thereof, in that manner. If the collection catheter 1412 is separate from the guide catheter 1404, the collection catheter with the clot treatment device 1202 is then pulled into the guide catheter for ultimate removal of all devices (and the clot) from the patient.
[0078] In certain circumstances, it may be advisable to remove the clot E without capturing it in the guide catheter 1404 or the collection catheter 1412 (if used) and remove the clot E by withdrawing the entire system, e.g., guide catheter 1404, delivery catheter 1406, clot treatment device 1202 and collection catheter 1412 (if used) simultaneously.
[0079] In several embodiments, the expandable portion 1414 the collection catheter 1412 is a conical funnel or tapered member constructed from a mesh, braid or stent structure. Such structure assists in retrieving and containing the clot material in the withdrawal process. In yet further embodiments, the collection catheter 1412 contains structural features to assist in the expansion of the funnel portion 1414 and to hold the funnel portion 1414 open towards the wall of the blood vessel. Such features (not shown) include interwoven support struts, self-expanding material (e.g., Nitinol), longitudinal wire supports, stent supports, polymeric webbing, etc.
[0080] In another embodiment of the present invention, a vacuum apparatus can be used to aid in the removal of the clot material. Referring to FIG. 16, a syringe 1602 is shown connected to a vacuum manifold 1606 that is in fluid communication with the proximal end of the guide catheter 1404. At the time the clot treatment device 1202 (and clot material) is being withdrawn into the guide catheter 1404 (or the collection catheter 1412), vacuum is applied by pulling on the syringe. Alternative sources of vacuum 1604 are also acceptable, e.g., a vacuum pump. A system is also contemplated whereby vacuum is actuated automatically when the clot treatment device 1202 (and the clot material) is being withdrawn. A representation of the effect of the use of vacuum can be seen with reference to FIG. 15B which shows how vacuum causes flow 1501 into the catheter 1412.
[0081] Referring now to FIGS. 17A-17H, alternative preferred embodiments of the clot treatment device 1202 are disclosed.
[0082] Referring to FIG. 17A, the capture portions 1206 between the generally cylindrical flow restoration portions 1212 of the clot treatment device 1202 are defined by a cylindrical disk shape with a rounded triangular cross-section.
[0083] Referring to FIG. 17B, the radially extending portions 1206 between the generally cylindrical flow restoration portions 1212 of the clot treatment device 1202 are defined by a cylindrical disk shape with a rounded triangular cross-section wherein the diameter of the disk increases along the length of the device 1202 thus forming a conical exterior extent.
[0084] Referring to FIG. 17C, the capture portions 1206 between the generally cylindrical flow restoration portions 1212 of the clot treatment device 1202 are defined by a cylindrical disk shape with a rectangular cross-section.
[0085] Referring to FIG. 17D, the radially extending portions 1206 between the flow restoration portions 1212 of the clot treatment device 1202 are defined by a cylindrical disk shape with a linear (non-rounded) triangular cross-section.
[0086] Referring to FIG. 17E, some of the capture portions 1206 between the generally cylindrical flow restoration portions 1212 of the clot treatment device 1202 are defined by a cylindrical disk shape with a rounded cross-section and others have a rectangular cross section.
[0087] Referring to FIG. 17F, the radially extending portions 1206 between the generally cylindrical flow restoration portions 1212 of the clot treatment device 1202 alternate between cylindrical disk shape with a T-shaped cross-section and a flare-shaped cross-section.
[0088] Referring to FIG. 17G, the radially extending portions 1206 between the generally cylindrical flow restoration portions 1212 of the clot treatment device 1202 are defined by a partial cylindrical disk shapes.
[0089] Referring to FIG. 17H, the radially extending portions 1206 between the generally cylindrical flow restoration portions 1212 of the clot treatment device 1202 are defined by tabs and bumps or protuberances arising from the cylindrical surface of the device 1202.
[0090] FIG. 18 is a cross-sectional view of another embodiment of the clot treatment device 1202 in accordance with the technology having an expandable member 1810, an elongated inner member 1820, and an elongated outer member 1822. The expandable member 1810 is configured to have an undeployed state in which the expandable member 1810 is elongated axially to have a low profile that fits within a delivery catheter as shown in FIG. 18. The expandable member 1810 is further configurable into a deployed state in which the expandable member 1810 forms a flow channel 1812 for restoring blood flow through the region obstructed by the clot. The expandable member 1810, for example, can be a mesh, braid, stent-type device, or other suitable member through which blood flows in the deployed state. In one embodiment, the expandable member 1810 is a continuous braid formed from a shape-memory material that has been heat set such that, in the deployed state, the expandable member 1810 has a plurality of flow restoration portions 1212 that expand to the first cross-sectional dimension D1 to form the flow channel 1812 and a plurality of radially extending portions 1206 that expand to the second cross-section dimension D2 greater than the first cross-sectional dimension D1. The flow restoration portions 1212 accordingly exert an outward force (arrows 0) against clot material (not shown) to create the flow channel 1812, and the radially extending portions 1206 accordingly exert a longitudinal force L (arrows L) against the clot material as the clot treatment device 1202 is moved proximally.
[0091] The elongated inner member 1820 can be a tube or coil having inner lumen configured to receive the guidewire 1402 for over-the-wire or rapid exchange delivery of the expandable member 1810 to the clot. The elongated outer member 1822 can be a tube or coil having a lumen configured to receive the elongated inner member 1820 such that the elongated inner member 1820 and/or the elongated outer member 1822 can move relative to each other along the longitudinal dimension of the clot treatment device 1202.
[0092] FIGS. 19 and 20 are detailed views of a distal portion 1901a (FIG. 19) and a proximal portion 1901b (FIG. 20) of the expandable member 1010 of the clot treatment device 1202 shown in FIG. 18. Referring to FIG. 19, the distal portion 1901a is attached to a distal end of the elongated inner member 1820 by the distal hub 1205. The distal hub 1205 can be blunt as described above with reference to the embodiment of the clot treatment device 1202 shown in FIG. 20, or the tip 405 can have a tapered distal portion 1840 configured to pass through the clot as shown in FIG. 19. Additionally, the distal hub 1205 can have a proximal opening 1842 configured to receive the distal end of the elongated inner member 1820 and the distal end of the expandable member 1810. Referring to FIG. 18, the proximal portion 1901b is attached to the distal end of the elongated outer member 1822 by a proximal hub 1830. For example, the distal and proximal portions 1901a and 1901b can be attached to the elongated inner member 1820 and the elongated outer member 1822, respectively, using welds, adhesives, crimping or clamping forces, and/or other suitable attachment mechanisms.
[0093] In the operation of the clot treatment device 1202 shown in FIGS. 18-20, the expandable member 1810 can self-expand from the undeployed state to the deployed state without an actuator. For example, as a delivery catheter is drawn proximally to release the expandable member 1810, the elongated inner member 1820 can be held in place to hold the distal portion 1901a of the expandable member 1810 distally of the clot. As the distal end of the delivery catheter moves proximally, the elongated outer member 1822 will slide distally as the expandable member 1810 expands until the expandable member 1810 reaches its predetermined deployed size or otherwise reaches equilibrium with the clot. In other embodiments, the elongated inner member 1820 and/or the elongated outer member 1822 can be actuators that are moved proximally and/or distally to control the radial expansion and/or the radial contraction of the expandable member 1810.
[0094] FIGS. 21 and 22 are detailed views of the proximal and distal portions 1901b and 1901a, respectively, of an expandable member 1810 and other components of a clot treatment device 1202 in accordance with another embodiment of the technology. In this embodiment, the clot treatment device 1202 has a proximal tube 2110 (FIG. 21) and an expansion element 2120 having one end attached to the proximal tube 2110 and another end attached to the distal portion 1901a (FIG. 22) of the expandable member 1810. The expansion element 2120, for example, can be a coil or spring that is stretched from its normal state when the expandable member 1810 is the low-profile, undeployed state inside the delivery catheter. As the distal portion 1901a and then the proximal portion 1901b of the expandable member 1810 are released from the delivery catheter, the expansion element 2120 contracts axially under its own stored spring force causing the expandable member 1810 to contract axially and expand radially outward.
[0095] In the embodiments where the expandable member 1810 is self-expanding, the expansion element 2120 assists the expansion of the expandable member 1810. In other embodiments, the expandable member 1810 may not be self-expanding or may be inherently spring-biased into the low-profile undeployed state, and the expansion element 2120 can have enough stored energy when it is stretched in the low-profile undeployed state to pull the distal portion 1901a and the proximal portion 1901b of the expandable member 1810 toward each other and thereby radially expand the expandable member 1810.
[0096] In the foregoing embodiments, the radially extending portions 1206 provide more surface area along the device than a device that is uniformly cylindrical. Moreover, the radially extending portions 1206 extend transversely to the longitudinal dimension of the device to more effectively transfer the axial force as the device is moved axially along the vessel after deployment. Such increased surface area facilitates the treatment and/or retrieval of a much larger portion of the clot E than is generally feasible with a uniformly cylindrical device. For example, in a preferred embodiment of the clot treatment device 1202, the device will have an external surface area between 1.5× and 6× the surface area of a uniformly cylindrical device of the same general diameter of the cylindrical flow restoration portions 1212. In other preferred embodiments the ratio can be 2× to 4×.
[0097] This can be advantageous particularly during retraction of the clot treatment device 1202 through the clot E. As shown in FIG. 14F, the clot treatment device 1202 may become elongated as it is being withdrawn through the clot E. Such elongation causes the clot material to encounter greater surface area of the clot treatment device 1202 than would otherwise occur with a device that was only generally cylindrical, e.g., that did not incorporate radially extending portions 1206. Accordingly the clot treatment device 1202 is particularly adept at capturing the maximum amount of clot material during withdrawal.
[0098] The clot treatment device 1202 is intended for use in large vessels, i.e., vessels with a diameter greater than 8 mm. For example, the diameter of the pulmonary arteries typically range from 15 to 30 mm whereas the first branches of the pulmonary arteries typically range from 10 to 15 mm and the secondary and tertiary branches typically range from 5 to 10 mm. At the same time, however, it is important to minimize the size of catheter providing access to the clot E. Accordingly, the clot treatment device 1202 has a large expansion ratio. In a preferred embodiment the expansion ratio from the diameter of the flow restoration portions 1212 in the collapsed state to the expanded state will be between 4 and 8. In another preferred embodiment the ratio will be between 5 and 7. The large expansion ratio also enables the formation of a flow channel in the clot E that is large, e.g., on the order of 4-8 mm.
[0099] The radially extending portions 1206, in their fully expanded position are intended to have a size that matches the diameter of the target blood vessel. However, the diameters may be slightly larger than the vessel diameter so to apply greater radial force against the blood vessel (without causing trauma) in those circumstances when it is desirable to improve clot collection. Similarly, in those circumstances where there is a concern of creating trauma on delicate blood vessels, the radially extending portions 1206 may have a diameter that is smaller than the vessel diameter. It is contemplated that different sizes of the device 1202 will be available for selection by the user for a particular presentation of the patient.
[0100] As for the length of the clot treatment device 1202, it is known that a typical pulmonary embolism will have a length within the range between about 2 cm and 10 cm and sometimes between about 1 cm and 20 cm. Accordingly, in a preferred embodiment, the clot treatment device 1202 will have a length that exceeds the length of the embolism so that a portion of the clot treatment device is positioned distal of the clot E during expansion.
[0101] With regard to the delivery catheter 1406, in a preferred embodiment for use with a pulmonary embolism, the size will be around 1 F-6 F. Smaller diameters will pass through the clot 100 more easily. In addition, the delivery catheter 1406 may have stiffness characteristics to assist in making sure the delivery catheter 1406 passes through the clot in a smooth manner. Such stiffness characteristics include self-expanding Nitinol wire braids or stent structures that are contained within the structure of the delivery catheter 1406. The delivery catheter 1406 also has sufficient flexibility so that it may carry the clot treatment device 1202 and still pass through a tortuous vessel path as described above starting with insertion of the delivery catheter 1406 in the femoral vein FV.
[0102] In some preferred embodiments, the method and device in accordance with the present invention may reduce the Mean Resting Pulmonary Artery Pressure (MRPAP). Upon at least partial relief from the clot 100, MRPAP may be reduced by about 20-50 mmHg to a normal range of 8-20 mmHg. In some embodiments, the reduction in MRPAP may be about 25-50%. In some embodiments, the reduction in MRPAP may be about 15% to 40% and in other embodiments between about 30% and 75%.
[0103] Such a reduction in MRPAP can occur in two steps. A first step is when the clot treatment device 1202 is first deployed and blood flow is at least partially restored. A second step may be when the clot treatment device 1202 is retracted and at least some of the clot E is removed from the vessel. A third step may be after the clot treatment device 1202 has been removed and the effect of the body's own processes and/or thrombolytic drugs that may have been used before, during or after the procedure take effect upon clot that has been disrupted by the clot treatment device.
[0104] FIG. 15 is a side view of an embodiment of a guide catheter 1500 for use with any of the foregoing embodiments of the clot treatment devices 1202 (not shown in FIG. 23). The guide catheter 2300 can include a shaft 2302 having a sufficiently large lumen to accommodate the delivery catheter 1406 (FIGS. 12 and 14A). The guide catheter 2300 can further include an expandable guide member 2310 at the distal end of the shaft 2302 configured to expand radially outward to contact or nearly contact the vessel wall VW. The guide member can be formed from a permeable, radially expanding material, such as a mesh or other macroporous structure (e.g., a braid of wires or filaments). The guide member 2310, for example, may be formed from a tubular braid of elastic or super-elastic filaments such as Nitinol that has been heat set into the desired expanded shape. The permeable, radially expanding guide member 2310 may have advantages over an occlusive member such as a balloon or impermeable funnel. For example, the guide member 1510 allows a substantial amount of blood flow BF to continue flowing through the blood vessel where therapy is being directed. In addition, the guide member 2310 positions the shaft 2302 and delivery catheter 606 at or near the center of the vessel. The clot treatment device 1202 (not shown in FIG. 23) may also be substantially self-centering upon deployment, and the guide member 2310 may further guide the clot material captured by the clot treatment device 1202 into the shaft 2302 as the clot treatment device 1202 moves into proximity of the distal end of the shaft 2302. This is expected to enhance aspiration of the clot material. For example, in the embodiment shown in FIG. 23, the radially expanding guide member 2310 has a funnel shape adjacent the distal end of the shaft 2302 to guide thrombus material into the distal opening of the shaft 2302 where it can be more readily aspirated.
[0105] The radially expanding guide member 2310 may also be formed by conventional machining, laser cutting, electrical discharge machining (EDM) or other means known in the art to make a fenestrated, mesh or porous structure that can be affixed near the distal end of the shaft 2302. In some embodiments the radially expanding guide member 2310 may self-expand, but in other embodiments it may be actuated by an operator using, for example, electrical or electromechanical means. By having a porous radially expanding guide member 2310, the guide catheter 2300 may be substantially centered within a vessel without blocking a large portion of the flow around the catheter. In some embodiments, the radially expanding guide member 2310 may block less than about 50% of the flow about the catheter and in other embodiments less than about 25% of the flow. When the guide member 2310 is made with a braid of filaments (e.g. wires), it may be formed from a tubular braid. In some embodiments, the tubular braid may be formed with approximately 12 to approximately 144 filaments, or in other embodiments from about 36 to about 96 filaments. The pores as measured by the largest circle that can be inscribed within an opening of the mesh may be between about 0.5 mm and 5 mm.
[0106] FIGS. 24 and 25 show additional embodiments of guide members 2410 and 2510, respectively, that can be used instead of or in addition to the guide member 2310. Referring to FIGS. 23 and 24, one or both ends of the tubular braid of the guide members 2310 and 2410 may be inverted and attached to the catheter body. Referring to FIG. 25, neither end of the guide member 2510 is inverted. With the distal end inverted, it advantageously may form a funnel adjacent the distal opening of the catheter that may enhance clot capture and aspiration.
[0107] FIG. 26 shows an embodiment of a guide catheter 2600 having a shaft 2602 and a guide member 2610 in accordance with another embodiment of the technology. In the embodiment shown in FIG. 26, the guide member 2610 has a tapered or funnel shape, and includes a non-permeable portion 2612 and a permeable portion 2614. The permeable portion 2614 can comprise a flared radially expanding mesh that has, at least in part, a tapered or funnel shape, and the non-permeable portion 2612 may have a substantially non-porous or otherwise non-permeable material or coating over the mesh. Preferably, the non-permeable material is a highly elastic material such as polyurethane, silicone, latex rubber and the like so that it can flex with the expansion of the mesh. In some embodiments, the non-permeable material covers a proximal portion of the mesh as shown in FIG. 26. The non-permeable portion 2612 may divert some flow away from the distal end of the catheter. The covering may cover a portion of the mesh to a diameter "d". In some embodiments, the diameter d of the covering is less than about 75% of the diameter "D" of the mesh funnel. In some embodiments, the diameter d may be less than about 50% of diameter D. The concept of a non-permeable material can also be applied to the guide catheter 2300 shown above in FIG. 23. For example, the expandable guide member 2310 of the guide catheter 2300 can have a non-permeable portion 2312 at the proximal portion of the expandable guide member 2310 similar to the non-permeable portion 2612 shown and described with reference to FIG. 26.
[0108] In any of the above embodiments shown and/or described herein, the clot treatment device and/or delivery system can be configured to facilitate maceration, fragmentation and/or disruption of the clot material. For example, unsheathing and re-sheathing the clot treatment device via advancement and retraction of the delivery catheter and/or the guide catheter can macerate the clot material held by the clot treatment device. As the guide catheter and/or delivery catheter slide across the outer layer of the clot material, the guide catheter and/or delivery member causes a repeated shear stress on the outer layer of the clot material that can weaken and/or fragment the clot and/or slough off outer layers of the clot. Moreover, retracting a clot having a larger diameter than the guide catheter and/or delivery catheter (or at the very least, having a portion that extends beyond the diameter of the guide catheter and/or delivery catheter) shears the clot material as it enters the guide catheter and/or delivery catheter, thus fragmenting the clot and releasing embolic particles from the main clot mass. In those embodiments where the clot treatment device and/or delivery system do not include a distal filter or embolic protection device, the released embolic particles are allowed to freely flow in the direction of the blood flow without being captured by a downstream device. It is expected that such restored blood flow causes natural lysis of the embolic particles.
III. Examples
[0109] Several examples of the present technology are as follows:
[0110] 1. A clot treatment device for treating a pulmonary embolism within a blood vessel, the clot treatment device being moveable between a low-profile undeployed state and a deployed state, the clot treatment device comprising:
[0111] a support member configured to extend through a delivery catheter, wherein the support member has a proximal portion and a distal portion;
[0112] a plurality of clot engagement members positioned circumferentially about at least an area of the distal portion of the support member, wherein individual clot engagement members have a curved portion;
[0113] wherein the clot engagement members are configured to penetrate clot material along an arcuate path and mechanically macerate clot material and release embolic particles when re-sheathed into the delivery catheter.
[0114] 2. The clot treatment device of example 1 wherein, in the deployed state, individual curved portions of the clot engagement members project radially outwardly relative to the support member in a curve that has a proximally extending section which defines a proximally facing concave portion, and wherein the individual curved portions further include an end section that curves radially inwardly from the proximally extending section.
[0115] 3. A method of treating a pulmonary embolism, comprising:
[0116] accessing a venous vessel of a patient;
[0117] inserting a catheter in the vessel and urging the catheter through the vessel, through chambers of the patient's heart and into a pulmonary artery until a distal end of the catheter is located at a region distal of a pulmonary embolism;
[0118] delivering a treatment device having a plurality of radially extending members through the catheter;
[0119] disturbing the embolus by mechanical maceration of the embolus to release embolic particles without capturing the embolic particles in an embolic protection device; and
[0120] establishing one or more blood flow channels through the embolus wherein the one or more blood flow channels facilitate natural lysis of the embolus.
[0121] 4. A method of treating a pulmonary embolism comprising:
[0122] delivering an embolectomy device through the heart to a pulmonary embolism that at least partially restricts blood flow through a pulmonary vessel, wherein the embolectomy device comprises an expandable cylindrical section and a radial expansion member configured to expand outwardly from the cylindrical section;
[0123] deploying the embolectomy device within the pulmonary embolism so as to restore blood flow through said pulmonary embolism,
[0124] wherein deploying the embolectomy device comprises expanding the cylindrical section within the pulmonary embolism such that the cylindrical section forms an expanded flow channel through the pulmonary embolism and expanding the radial expansion member to a greater extent than the cylindrical section, and wherein at full expansion of the cylindrical member the radial expansion member projects outward from the cylindrical member;
[0125] fragmenting the pulmonary embolism while moving the embolectomy device and at least a portion of the pulmonary embolism along the pulmonary vessel; and
[0126] withdrawing the embolectomy device and at least a portion of the pulmonary embolism from the pulmonary vessel.
[0127] 5. A device for treating a pulmonary embolism that at least partially restricts blood flow through a pulmonary vessel, the device comprising:
[0128] an elongated shaft having a proximal region and a distal region;
[0129] an expandable braid attached to the distal region of the elongated shaft, the braid having a plurality of radially extending portions and at least one cylindrical portion, and the radially extending portions and the cylindrical portion being configured to move from a compressed state sized to fit in a delivery catheter to an expanded state;
[0130] wherein the cylindrical portion is between a pair of the radially extending portions, and in the expanded state the cylindrical portion is configured to press radially outward against the pulmonary embolism;
[0131] wherein the radially extending portions extend radially outward from the cylindrical portion in the expanded state such that portions of the pulmonary embolism are retained between the radially extending portions; and
[0132] wherein the cylindrical portion has a first length along a longitudinal direction of the braid in the expanded state and the radially extending portions have a second length along the longitudinal direction of the braid in the expanded state that is less that the first length; and
[0133] wherein the radially extending portions and/or the cylindrical portions are configured to elongate and/or contract when re-sheathed into the delivery catheter to mechanically macerate clot and release embolic particles.
[0134] 6. The device of example 1 wherein at least a portion of the individual radially extending portions is disk-shaped.
[0135] 7. The device of example 1 wherein the individual radially extending portions include a curved portion and a linear portion.
[0136] Although the invention has been described in terms of particular embodiments and applications, one of ordinary skill in the art, in light of this teaching, can generate additional embodiments and modifications without departing from the spirit of or exceeding the scope of the exampled invention. Accordingly, it is to be understood that the drawings and descriptions herein are proffered by way of example to facilitate comprehension of the invention and should not be construed to limit the scope thereof.
User Contributions:
Comment about this patent or add new information about this topic:
Images included with this patent application:
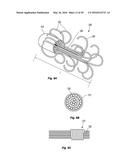 | 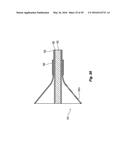 |
 |  |
 |  |
 |  |
 |  |
 |  |
 |  |
 |  |
 |  |
 |  |
 |  |
 |  |
 |  |
 |  |
 |
| Similar patent applications: | |
| Date | Title |
|---|---|
| 2010-09-23 | System and method for treating tumors |
| 2016-01-28 | Respiratory assembly |
| 2016-02-11 | Medical apparatus |
| 2016-03-24 | Percutaneous heart pump |
| 2016-03-17 | Modulated drug delivery |
| New patent applications in this class: | |
| Date | Title |
|---|---|
| 2019-05-16 | Otoscope tip and methods of use |
| 2019-05-16 | Scanning of cavities with restricted accessibility |
| 2016-06-02 | Medical instrument with probe and methods of using the same |
| 2016-05-12 | Medical diagnostic instrument |
| 2015-12-10 | Otoscope |
| New patent applications from these inventors: | |
| Date | Title |
|---|---|
| 2022-08-11 | Braiding machine and methods of use |
| 2022-08-04 | Single insertion delivery system for treating embolism and associated systems and methods |
| 2022-07-07 | Hemostasis valves and methods of use |
| 2022-07-07 | Device and method for treating vascular occlusion |
| Top Inventors for class "Surgery" | |
| Rank | Inventor's name |
|---|---|
| 1 | Roderick A. Hyde |
| 2 | Lowell L. Wood, Jr. |
| 3 | Eric C. Leuthardt |
| 4 | Adam Heller |
| 5 | Phillip John Plante |